Posted by admin …
Bring On the Death Panels | April 5, 2016
One of the things I hear patients talk about when they mention Obamacare is the “death panels”..as they sneer these words they look to me for some knowing and indignant nod of agreement at this latest oppressive government outrage.
 Unfortunately, they are again disappointed in me because I stop them in their tracks when I intone…”We need the death panels…the death panels are a very good idea…I’m all about the death panels !”
Unfortunately, they are again disappointed in me because I stop them in their tracks when I intone…”We need the death panels…the death panels are a very good idea…I’m all about the death panels !”
The term “death panel” conjure up some white coated tribunal of indifferent doctors ..hired guns as it were …strangers who will chose who lives and who dies. Which grandma still has a little life in her yet. Whom to refuse fourth line chemotherapy. Which sick little baby will be tossed off the side of the mountain as the ancient Spartans used to do with children who did not seem whole and well. Cruel, Arbitrary and Indifferent ! Who could be comfortable with those decisions?!
Swap out the word “independent” for “ indifferent “ and I am actually down with the plan. You will be as well once I have explained things from my standpoint. When you really think about it, and I don’t blame you if you haven’t been preoccupied with this subject… who better than to decide on your medical fate than a professional medical team of independent experts. This isn’t about the death panel randomly picking out people at Destiny USA for harvesting like some grim reaper Halloween pageant. This whole issue is about what to do at the end of meaningful productive life. This is about not torturing Grandma during her final days despite the well meant desires of their family.This is not just about what makes economic sense. Frankly I think economics should not factor into the equation in any way shape or form at all but you can’t be ignorant of the financial issues. WNET news reports that “Medicare, the health insurance program for the elderly, spends nearly 30 percent of its budget on beneficiaries in their final year of life. Slightly more than half of Medicare dollars are spent on patients who die within two months.” That’s a staggering amount of money and sadly it’s usually poorly spent. Way too many grandmas spend their last few days on Earth in some oddly lit room full of strangers and stranger equipment…often tied up to the bed or some equipment , sedated lest they pull on their life support. One tube going in here and another tube coming out there Never well enough to have meaningful communication with their family. Dragging out the inevitable process from hours to days if you allow nature to take its course to weeks or even longer if “all measures are taken” to keep grammie going . I’m sorry but that’s just not right!
 Although I am sure Obamacare’s underlying concerns are financial I view the Death Panels from a more moralistic standpoint. Sometimes enough is enough. Just because you can artificially prolong someone’s life doesn’t mean you should. My sister who is a doctor in Florida once approached my mother with consternation and although I wasn’t there I imagine a little indignation as well…”Mom” she decried .” Do you know that your health care proxy…your first born son ….Bud..(meaning me) ….has told us that if you were demented and in a nursing home and had pneumonia ….he would withhold antibiotics ..he would just let you die ! “ My mother responded ….”That’s precisely why HE is my proxy and YOU are not ! “ I know Momma wouldn’t want to be kept alive under those circumstances…and I have the conviction to honor HER wishes. Not impose my own.
Although I am sure Obamacare’s underlying concerns are financial I view the Death Panels from a more moralistic standpoint. Sometimes enough is enough. Just because you can artificially prolong someone’s life doesn’t mean you should. My sister who is a doctor in Florida once approached my mother with consternation and although I wasn’t there I imagine a little indignation as well…”Mom” she decried .” Do you know that your health care proxy…your first born son ….Bud..(meaning me) ….has told us that if you were demented and in a nursing home and had pneumonia ….he would withhold antibiotics ..he would just let you die ! “ My mother responded ….”That’s precisely why HE is my proxy and YOU are not ! “ I know Momma wouldn’t want to be kept alive under those circumstances…and I have the conviction to honor HER wishes. Not impose my own.
That’s always one of my founding principles…do what the patient would want…not what I would do or what the family wants….What would the patient want had they still had the capacity to tell us? WWMW..What would Momma want ? That actually makes it easier for me. I feel better when I am honoring the known wishes of the patient. Having said that I also feel there is a place for an independent evaluation of the end of life situation.
There comes a time…and it’s almost always involving the hospital…when the question has to be raised ….Are we doing too much? Have we gone too far?.. I think there is a place for an independent panel to weigh in on this issue. If it’s obvious that we are dealing with a possible end of life issue I think we should call a “Code White” Although we can work out the details later it would be, I think, relatively easy to convene a panel of independent doctors who can evaluate the situation and the patient and weigh in on the appropriate use of advanced life support. Mind you these people would never have the last say in what happens to the patient but they would determine whether insurance of any kind should pay for the care.
 So I could envision this scenario…..Your mother has advanced dementia and hasn’t been able to say the names of her kids in years or live independently. She gets pneumonia and is hospitalized. She does poorly despite usual hydration and antibiotics…and the questions become….should she go to the ICU for closer monitoring?…should she be fed by a tube since she is not eating well? ….How many tests and procedures to put her through ? CODE WHITE …is called an within a day a panel of doctors would have reviewed the chart and examined the patient and would be able to weigh in as to what’s the most appropriate thing to do. At that point they would not say what could or could not be done but would say what would be covered by insurance. It’s OK to say “Keep Momma alive at all costs !” But it’s also OK for a panel of experts to say …”We feel that aggressive care is not appropriate but It’s fine if you want to proceed but it’s not going to be covered by insurance and its 5,000 dollars a day for the ICU and can we have 3 days stay in advance.?!” . Of course there is the risk that these oversight doctors will be incentivized to cut short care to reign in finances but what we have now is just as bad….No cost control whatsoever and even worse …no routine evaluation of the appropriateness of care. You rightly fear a government that will devalue lives but I see every day where we , from an understandable combination of love and regret and fear , put our loved ones through procedures that rob them of their dignity and deny them a comfortable reflective peaceful passing. We can do better…we must do better and the Death Panel conversation is a good place to start.If this article does nothing else but get you to make sure Momma has a Health Care Proxy and someone both knows what Momma wants but has the strength to carry out HER wishes then I have been of service…
So I could envision this scenario…..Your mother has advanced dementia and hasn’t been able to say the names of her kids in years or live independently. She gets pneumonia and is hospitalized. She does poorly despite usual hydration and antibiotics…and the questions become….should she go to the ICU for closer monitoring?…should she be fed by a tube since she is not eating well? ….How many tests and procedures to put her through ? CODE WHITE …is called an within a day a panel of doctors would have reviewed the chart and examined the patient and would be able to weigh in as to what’s the most appropriate thing to do. At that point they would not say what could or could not be done but would say what would be covered by insurance. It’s OK to say “Keep Momma alive at all costs !” But it’s also OK for a panel of experts to say …”We feel that aggressive care is not appropriate but It’s fine if you want to proceed but it’s not going to be covered by insurance and its 5,000 dollars a day for the ICU and can we have 3 days stay in advance.?!” . Of course there is the risk that these oversight doctors will be incentivized to cut short care to reign in finances but what we have now is just as bad….No cost control whatsoever and even worse …no routine evaluation of the appropriateness of care. You rightly fear a government that will devalue lives but I see every day where we , from an understandable combination of love and regret and fear , put our loved ones through procedures that rob them of their dignity and deny them a comfortable reflective peaceful passing. We can do better…we must do better and the Death Panel conversation is a good place to start.If this article does nothing else but get you to make sure Momma has a Health Care Proxy and someone both knows what Momma wants but has the strength to carry out HER wishes then I have been of service…
Until next month…get well …stay well….
Let’s Roll | March 7, 2016
Dr. Barry
I am wincing as I type this….no, not from my painful turn of prose…I took a beating in the dojo where I attempt to learn jujitsu. Well, the truth is I take a regular beating there but this one taught me a lesson. Hopefully only a temporary pain but a long remembered lesson. I love jiu jitsu… it’s like adult wrestling and chess mixed together.
…and the workouts where you spar / grapple / roll even for 3 minutes can leave me feeling exhausted. I love that feeling. If I am going to work out I want to feel beat afterwards. Jiu-Jitsu_Brasileño Now let me admit that I am terrible at jujitsu as my attendance has been less than stellar this last year. When you don’t practice often enough it’s hard to remember the right moves and counters. I know that if I go more often that has to help. Since in my profession I exhort my patients to work out more regularly I thought it would be wise to practice what I preach and make jujitsu attendance a bigger and more regular part of my routine. So,I set my schedule for twice a week. Between twice a week at the dojo and my biweekly sax lessons I am bound to improve myself somehow and someway. So there I was at class last friday. rolling with a guy less than half my age, twice my strength, and much higher belt level. I knew this guy doesn’t roll lightly. But I’m there for the challenge and besides when you are as old as I am, relative to the rest of the class…and as inexperienced as I am ..pretty much everyone is better than me and I am bound to get whooped each and every time. My ego can take it and it’s always great exercise and hopefully I am slowly getting better. I like it when my opponent has a serene look…this one guy wouldn’t recognize serene if he saw it in a magazine. Maybe it’s my innate paranoia but I get a subtle “ I’m not going to get much out of rolling with this guy..it’s a waste of my time “. That’s absolutely true…!! .I have watched him roll, he is very good and goes hard so I understand where he is coming from. During our roll he actually took it easy on me and I think that might have pissed him off even more because even when he went easy it was hard for me to sustain an attack or defend myself. During just one of the many times he was choking me or using an arm bar I might have resisted a bit too much for too long and got myself in a position where my opponent was locking my arm up to make me quit. Whenever you feel you have been bested and are ready to admit defeat and start again all you have to do is tap the other guy and they will let up. When people don’t tap they are telling you to use more pressure, better technique etc before they will admit defeat. So when I didn’t tap immediately the higher belt took it to a higher level and we could both feel when I hyperextended my elbow. It didn’t get dislocated just stretched a wee bit more than usual. It felt funny for a second then everything was back to normal and we continued the three minute session. I rolled with two more guys before I staggered off the mat. It was only later while driving home that it started to hurt. I knew nothing was broken …just painful. It was very tender today but there is still fullish range of motion and terrible swelling or bruising so let’s see how it goes before I go running off to the doctor. As long as it gets a little better each day I will just follow it. I had already learned long ago that active people will get injured. You can’t stop because of injury …you have to modify. This elbow thing will not allow me to use the rowing machine so I will spend more time on the bike and ski machine. No the lesson I learned this time was to TAP EARLY! Don’t be all macho on the mat…When you know you have been beaten… accept defeat and move on. Leave the dislocations to someone else…anyone else. I am not normally a guy that says “Know your limits.” How can you know your limits without testing them? Don’t sell yourself short. I try to remember this is a marathon not a sprint. If I resist too much and get hurt that affects my overall ability to train. Recurrent injuries have made many a person finally give up their sport. If I take it a little easier I can stay in the game longer. Let’s see if the other guy is still rolling when he is my age.! Jujitsu is one of the few sports you can do at any age…you don’t see a lot of guys playing baseball, basketball, soccer or football as they get past 40 years of age…but you can “roll” on the mats until an advanced age if you have the desire. I hope you have some physical activity you can keep interested in through all phases of your life. Until next month…get well …stay well…and when you get injured regroup and get back in the game !
MAKING A DIFFERENCE WITH A WORD CLOUD | Feb 7 2016
Dr. Barry
Well, It’s February and that means Valentine’s Day is around the corner. Hopefully you are not expecting “that column” The one where I say how important sex is to men and how easy it is to make us happy. Before the cat calls of chauvinism start I am only echoing the sentiment of Dr. Ruth, Dr. Laura, and the girl from friends.
RFH_WordCloud2No, love is an easy subject which you will be saturated with on the radio, TV, newspapers etc. Writing about love and sex ..two different but important topics …that’s the low hanging fruit…too easy for me. Been there done that. Well perhaps just one suggestion…use oil…use lube ..it works on the feet, it works on the neck and it works on the tender bits. It can really make a difference.
Speaking of making a difference I am writing this week to bring to your attention the idea of a WORD CLOUD for someone who is sick and or dying. OK, pay attention, this is important for a change. Most of you will turn from this. I don’t blame you… it’s a tough and touchy subject .Perhaps just one amongst you will follow the advice in this column and that would be worth it .That would make a difference. I know it’s not an easy subject but it’s an important one. elderly-hospital-patient-1437289
I write today about word clouds. Specifically, word clouds for people who are very ill. Let me explain…this is not an original idea on my part. This comes from an article printed in the Annals of Internal Medicine last year. Listen, serious illness, death and dying are tough to write, read and talk about but it’s important and can make a big difference. The full article involved transitioning the patient from the medication and procedure centric focus to focusing more on the wishes of the ill patient. Basically you have a frank conversation with the patient…The last chapter of your life is being written…you can tell us what’s important to you and what you want to accomplish before the last page is turned. “I want to see my nieces again” “I want to reconcile with my ex sister in law” “I want to get in the garden again and surround myself with the sights and smells of the flowers” “I want to have this music play at my funeral etc”. This is difficult stuff and many people shy from it…both health care professionals and patients and family alike.
words-639306A word cloud is basically a message board. It’s a framed collage of words as a keepsake for the patient AND family and friends. You bring a board you can write on…Put the patient’s name prominently in the middle and have staff, friends and family mark it up as they see fit. People can add special expressions or pet sayings or phrases…something that connected them to the patient. The word cloud prompts recollection and reflection. Family sees and contributes …Friends see and contribute. This connects everyone to everyone else. This gives people a focus point for conversation when they come in the room. It gives you something else to focus on other than the hospitalization and illness itself. Visiting patients in the hospital …especially seriously ill patients can be very uncomfortable for people. This is a way to focus the conversation away from illness and towards the patient and their shared memories. It doesn’t have to be just “how’s the food” and long awkward silences. Instead you can focus on the Cloud Board ..“I wonder who wrote that !” “I wonder what this means?” When the hospital staff see such a visual expression it acts to remind them that it’s not just another body in the bed…it’s a “touchstone to appreciate the footprint of the patient’s life and to learn what mattered most to the patient.”Doctor_consults_with_patient_(4)
Let’s say the patient improves and goes home…they have a great memento of the experience with real comments from real people about themselves. Not just an inexplicable hospital bill. Let’s say the patient succumbs from their illness…the family has a one of a kind memento of the patient which can be brought to any service they might have …and can serve as a visual remembrance for years to come. Flowers fade. Notes get put in some drawer. This word cloud will long serve as a reminder of the patient and who they touched in their lives. I sent an example along with this article that hopefully they can reproduce to give you a better idea of what I am talking about…a picture is worth a thousand words they say .
As a doctor I struggle with the idea of making a difference in someone’s life. I struggle too with making a difference in someone’s death or serious illness. With this word cloud idea I think I can make a real impact in how people deal with the process. You can too. This doesn’t have to come from the doctor. In fact I don’t ever see this coming from the doctor or staff so it’s up to you! You CAN make a contribution during this difficult time…a contribution that will stand the test of time. Go, make a real difference. I’ll be here when you get back.
Get Out! Is It Christmas Already? | Dec 2015
Dr. Barry
 GET OUT! Is it Christmas time already? It’s a wonderful time of the year but it’s very stressful for a lot of people. The traveling. The shopping. The scheduling. What to get for who. It is a very busy time for most people. Busy busy busy but it’s important to stop and take stock for a moment.
GET OUT! Is it Christmas time already? It’s a wonderful time of the year but it’s very stressful for a lot of people. The traveling. The shopping. The scheduling. What to get for who. It is a very busy time for most people. Busy busy busy but it’s important to stop and take stock for a moment.
Dare I say be mindful? When people are “busy” they are getting stuff done but they are usually not thinking much. Not thinking about their lifestyle. Not thinking about what’s really important during this Holiday season. I love the line from Dickens’ A Christmas Carol where Scrooge is confronted by the ghost of his long dead partner Jacob Marley … Scrooge complimented him on his business acumen when alive and the ghost remonstrates, “Mankind was my business. The common welfare was my business; charity, mercy, forbearance, benevolence, were all my business. The dealings of my trade were but a drop of water in the comprehensive ocean of my business!” His trade was not his business! Let me help. Let me give you a couple of ideas for the holidays. First…the gift of massage…Get someone you love a gift certificate to massage therapy.
 It’s the antidote to busyness. There are a few people out there who don’t like massage and we are rounding them up for analysis but they can always re-gift the certificate. The nice thing about the gift certificate is that the person you give it to can arrange when they want the massage…It doesn’t add to the scheduling stress of the holiday. Also, consider the gift of a yoga class…nothing is more relaxing and revitalizing as a yoga class…you might not have thought of this as a gift idea but it’s a good one…for an interesting variation that even my wife liked…try Aerial Yoga! Even your friends that have everything or have tried everything will have been unlikely to have tried this yet. Lest I leave the wrong impression…my wife is super easy to please…she just doesn’t find regular yoga strenuous enough…not enough sweating for her hour of exercise…She was, however, very impressed by the aerial yoga.
It’s the antidote to busyness. There are a few people out there who don’t like massage and we are rounding them up for analysis but they can always re-gift the certificate. The nice thing about the gift certificate is that the person you give it to can arrange when they want the massage…It doesn’t add to the scheduling stress of the holiday. Also, consider the gift of a yoga class…nothing is more relaxing and revitalizing as a yoga class…you might not have thought of this as a gift idea but it’s a good one…for an interesting variation that even my wife liked…try Aerial Yoga! Even your friends that have everything or have tried everything will have been unlikely to have tried this yet. Lest I leave the wrong impression…my wife is super easy to please…she just doesn’t find regular yoga strenuous enough…not enough sweating for her hour of exercise…She was, however, very impressed by the aerial yoga.
Second…the gift of your company. Take your aunt out to one of the seasonal events…Maybe you have done Lights on the Lake one time too many…still plenty of other venues for you. Take them outdoor skating downtown. Not very expensive but it will be a memorable experience for everyone. Take them for a horse driven carriage or sleigh ride at Highland Forest…being on the sleigh covered with a blanket as you glide along the pathway with the twinkling of the stars competing with the jingling of the bells on the horses…memory magic! Let me recommend the Desantis Xmas at the Palace show. Hearing seasonal music done by live local talent in this great venue never gets old to me.
 Often, they have talented kids from the local schools perform and that’s bonus time! This is a great show for the young and old and everyone in between. The popcorn made fresh in the lobby is another draw for me. My office is one of the sponsors for this show and we never miss it!
Often, they have talented kids from the local schools perform and that’s bonus time! This is a great show for the young and old and everyone in between. The popcorn made fresh in the lobby is another draw for me. My office is one of the sponsors for this show and we never miss it!
Also, the Winter Solstice Celebration is coming back to Syracuse. This show will be at St Paul’s Cathedral downtown and run for 3 4 nights. When the Solstice Celebration was last in town it was an eclectic mix of solemn, seasonal, and joyful music. You will leave the Cathedral uplifted and how many events can you say that about!! There is so much more to recommend…Spend an afternoon snowshoeing or X country skiing with family or a friend. Being outdoors in this weather is very very good for you…it increases your metabolism and helps you burn off some of those Christmas goodies. Bottom line is that this holiday should be about you growing your personal relationships not your relationship with Amazon Prime. Merry Christmas and Happy Holidays to one and all.
The Fast Track | November 3, 2015
Dr. Barry
 I have studied diabetes for years…all primary care doctors have…but only recently have I been exposed to a concept that can really make a difference in the care of diabetics. One of my Signature MD patients sent me a link to Dr Jason Fung …a doctor with a “new” approach to treating type 2 diabetes. Immediately, I saw the rightness of the idea. There have been multiple new drugs in the past several years but they just increase our medication choices…they don’t have a meaningful impact on changing the lives of diabetics. When you become a diabetic you go on one med…after a bit you go on a second med…eventually many people go on an injectable agent…all the while monitoring their sugars, blood pressure and cholesterol levels routinely. We are treating the sugar number but not the underlying problem which is that your insulin levels are too high.
I have studied diabetes for years…all primary care doctors have…but only recently have I been exposed to a concept that can really make a difference in the care of diabetics. One of my Signature MD patients sent me a link to Dr Jason Fung …a doctor with a “new” approach to treating type 2 diabetes. Immediately, I saw the rightness of the idea. There have been multiple new drugs in the past several years but they just increase our medication choices…they don’t have a meaningful impact on changing the lives of diabetics. When you become a diabetic you go on one med…after a bit you go on a second med…eventually many people go on an injectable agent…all the while monitoring their sugars, blood pressure and cholesterol levels routinely. We are treating the sugar number but not the underlying problem which is that your insulin levels are too high.
am talking now about the very common type 2 diabetes not the uncommon type 1 diabetes where they don’t make enough insulin. So, most diabetics have insulin resistance and high insulin levels. High insulin levels prevent you from burning fat, High insulin levels cause weight gain. High insulin levels keep your belly fat growing. High insulin causes salt retention and therefore raises blood pressure. So, high insulin levels bad. Now the current diabetic teaching is low carb, frequent small meals etc… Not bad advice but no where near the best advice for treating high insulin levels. To treat diabetes and prediabetes effectively you must get the insulin level lower. Turns out that this is possible and doesn’t require any strange new meds, treatments or therapies.
 Ok, how much extra time in your day do you need for this new treatment? How much money will it cost? How many choices will you have to make each day? Special equipment? Extra doctor or professional visits? The short answers are that it frees you from too many choices. It will save you time. It will save you money. No special meetings or equipment needed. Do I have your interest piqued yet? Well, I am talking about intermittent fasting. Fasting lowers your insulin level back to normal. This allows you to start mobilizing the fat in your body. Fasting reverses all the metabolic processes that insulin resistance causes.
Ok, how much extra time in your day do you need for this new treatment? How much money will it cost? How many choices will you have to make each day? Special equipment? Extra doctor or professional visits? The short answers are that it frees you from too many choices. It will save you time. It will save you money. No special meetings or equipment needed. Do I have your interest piqued yet? Well, I am talking about intermittent fasting. Fasting lowers your insulin level back to normal. This allows you to start mobilizing the fat in your body. Fasting reverses all the metabolic processes that insulin resistance causes.
There are many many types of fasts…I have gently recommended the 5:2 diet for years….5 days a week you eat healthy…2 days a week you take in only 500 calories or less. This is simple, basic and reasonable. I recommend doing the two days in a row for best results but you can vary the schedule to suit you. The intermittent fast recommended by Dr Jason Fung involves skipping breakfast and lunch every day and only taking in calories from 6 10 pm at night. Yes, this flies in the face of all the recommendations that you should eat a big breakfast and or have 5 small meals a day. If you follow that advice, you will keep spiking your insulin and weight loss will be much harder. This advice certainly has not made a dent in our diabetic problem or obesity problem. With intermittent fasting you don’t have to make a decision as to what to eat for breakfast or how to manage eating lunch on the road etc.… You don’t have to spend extra time in the gym, buy special scales or tubs, or learn anything new about calories, fats, protein etc. The first few times are psychologically daunting but almost UNIVERSALLY people that do the intermittent fasting FEEL BETTER. More energy. More mental focus. Less stomach issues. As the doctor said on one of the many videos I reviewed for this issue, you can do the test of 1. That is , try it for yourself ..you be the judge. You don’t have to ask anyone else what happened to them or how they feel. You can try fasting for yourself and see for yourself and feel for yourself the benefits. “Oh I could never fast…it’s just too hard !” Really? A billion people fast for Ramadan, Hindus, Buddhists, and old fashioned Catholics all have experience with fasting.
 I am not going to give you the play by play because it really is just that simple…black coffee and water only until 6 pm. Eat healthy or not for 4 hours then no food after 10 pm. There are many variations on the Internet. Start with Dr Fung on youtube and off you will go. By the way…this is not really some new fad or trend. Fasting has been around as long as we have. When people tell me that it’s impossible to do I refer them to the TV show…Naked and Afraid ..where strangers are put together in the wilderness for 21 days to survive. The vast majority of them never find anything to really eat and that has not prevented anyone from completing the challenge. They might get sick from drinking contaminated water but no one quit due to lack of calories.
I am not going to give you the play by play because it really is just that simple…black coffee and water only until 6 pm. Eat healthy or not for 4 hours then no food after 10 pm. There are many variations on the Internet. Start with Dr Fung on youtube and off you will go. By the way…this is not really some new fad or trend. Fasting has been around as long as we have. When people tell me that it’s impossible to do I refer them to the TV show…Naked and Afraid ..where strangers are put together in the wilderness for 21 days to survive. The vast majority of them never find anything to really eat and that has not prevented anyone from completing the challenge. They might get sick from drinking contaminated water but no one quit due to lack of calories.
You don’t have to need to lose weight, you don’t have to be a diabetic, you just have to want to feel better. If you are a diabetic on lots of meds it would be prudent to check with your doctor about which meds to cut back etc. Your doctor should be sympathetic to your efforts even if he is not familiar with fasting. If he can’t be bothered perhaps it’s time to upgrade your medical care. When I mentioned fasting to one of my colleagues he opined that he thought the idea made sense but that we couldn’t get people to go along with it. I have more faith in you than that.! Did I mention that people who do fast say they feel physically and mentally better!
Let me close with a few quotes about fasting so you know it’s not just me! “Humans live on one quarter of what they eat; on the other three quarters lives their doctor.” Egyptian pyramid inscription, 3800 B.C. “Fasting is the greatest remedy the physician within.” Philippus Paracelsus, one of the three fathers of Western medicine “Instead of using medicine, better fast today.” Plutarch, a Greek biographer and moralist “The best of all medicines is resting and fasting.” Benjamin Franklin Until next month…get well stay well…
Preach, Practice, Repeat | October 6, 2015
Dr Barry
I am trying to practice what I preach…I have always believed that good living will trump most medications. I am not saying you can treat all medical problems with diet and exercise but I am saying that lifestyle is more important than medications.
 Look up the treatment recommendations for hypertension, heart disease, diabetes, arthritis, etc and the first line will say either diet and exercise or lifestyle modification which is really the same thing. Your doctor glosses over this because he or she has no control over what you eat or whether you work out…What we in the medical profession can control are the meds and you know we love our pills! We give out pills to help you sleep at night and then another pill to keep you awake during the day. One pill for your blood pressure and another to counteract the side effects. When you add in the supplements and the vitamins and aspirin many people find they are taking 10 pills a day or more. We can’t control you but we can control the pills we give you.
Look up the treatment recommendations for hypertension, heart disease, diabetes, arthritis, etc and the first line will say either diet and exercise or lifestyle modification which is really the same thing. Your doctor glosses over this because he or she has no control over what you eat or whether you work out…What we in the medical profession can control are the meds and you know we love our pills! We give out pills to help you sleep at night and then another pill to keep you awake during the day. One pill for your blood pressure and another to counteract the side effects. When you add in the supplements and the vitamins and aspirin many people find they are taking 10 pills a day or more. We can’t control you but we can control the pills we give you.
So, my mantra has been diet and exercise…exercise and diet…I read somewhere that to get the same benefit a person gets from statin drugs (the popular cholesterol lowering drugs like crestor, lipitor, zocor etc ) …the radical alternative that has the same benefit as the statins….eat more veggies ! Now I am talking about primary prevention here… If you have already had a heart attack, blocked arteries, stents, stroke, diabetes etc that’s secondary prevention and the statins are very important for those people.
The debate has raged however as to how important it is for the average Joe to take a statin. Some doctors think they are overprescribed while other doctors think practically everyone should be on a statin. The studies are reviewed all the time with different conclusions depending on who is doing the interpretation. The most recent recommendation regarding statin use involves using a risk calculation like https://cvdrisk.nhlbi.nih.gov/..If your 10-year risk is higher than 7.5% you should consider a statin. This number is calculated by putting in your sex, your age, your cholesterol number, smoking status , and blood pressure information.
So, I try to plug in my numbers and when I punch the calculation button I get an error message. It seems my cholesterol level is so high that the computer assumes that I mistyped the number. My cholesterol is so high that when I tried to get life insurance years ago the agent said…don’t bother to even apply. My response at the time was to show them my recent cardiac cath results which did not show any blockage. So even though my cholesterol was high…it was not sticking to my arteries. They didn’t care that I didn’t have blocked arteries …they only cared about the number on the paper…So I went on meds…got my number to where they wanted it and got my insurance. Of course I stopped the pills afterwards…I am not a pill guy if I can help it.
 Fast forward to this month…From time to time I get chest symptoms. Could be anything…probably nothing but that’s not how I treat my patients. If you worry about some symptom and some test can give us information why not get the test? At least twice a year I will push myself past the limits of my endurance physically…usually hiking and skiing with the Clan Haswell. I would rather not keel over in the near future because life is great right now. My wife still seems interested in me and my professional work has never been more satisfying with Signature MD so I would like to stick around long enough to at least see how Iran, Greece and China all play out.
Fast forward to this month…From time to time I get chest symptoms. Could be anything…probably nothing but that’s not how I treat my patients. If you worry about some symptom and some test can give us information why not get the test? At least twice a year I will push myself past the limits of my endurance physically…usually hiking and skiing with the Clan Haswell. I would rather not keel over in the near future because life is great right now. My wife still seems interested in me and my professional work has never been more satisfying with Signature MD so I would like to stick around long enough to at least see how Iran, Greece and China all play out.
I told you that I took meds to get my cholesterol down…I didn’t stay on the meds…I don’t like meds and what I read says you can accomplish the same thing with the right diet and exercise program so that’s what I concentrate on. But am I being stupid not treating my high cholesterol? Are my arteries slowly and silently clogging up? In my favor is the fact that I am not a smoker or a diabetic ..that makes whatever cholesterol you have stickier. Also, my family history is good…neither parent having had an mi or stroke. So , do you go with a good family history and lifestyle or go with the population based scientific calculation. Well, you don’t have to be abstract about it…you can just measure the amount of blockage and act accordingly. So, last month, I went to St Joseph’s Hospital and had a heart catheterization. They snake a wire from your wrist or groin to your heart and inject dye to check the arteries. It’s an interesting sensation. Not pleasant but tolerable. Dr Simon and his team were very professional …not even giving me grief about my not wanting to take any sedating meds. I don’t like to alarm my wife and I figured if I skipped the sedating meds I could drive myself home. My wife is a working girl after all and no need to keep her from her job. Bottom line is that there were no real blockages. Maybe a little plaque here and there but no blockages that needed stents, balloon angioplasty etc. If that’s all the blockage I have after 57 years of genetically high cholesterol I am doing the right things!! Maybe the tequila has some role in keeping the arteries open but that’s another column altogether. Until we know for sure I am going to credit the exercise and diet. I feel a little vindicated with my diet and exercise mantra. I also think having a persistently optimistic attitude is also important but that may be more for my head than my heart. There is data to suggest that being happy…having a positive attitude ..is as important for your heart as it is for your head and I want to believe that as well.
The deal I made with the heart doctor was that if there was any plaque at all …any narrowing…I would go on the statins. I don’t like statins but a deals a deal. If they will only come up with a pill I could take Sundays only…that way I could be possibly compliant with doctors’ orders. Just because I think I am a good doctor doesn’t make me necessarily a good patient!
So, just like I preach and practice…if you worry about a possible problem and there is a test for it…why not find out for sure. You know I don’t like surprises or guessing. When it comes to your health you shouldn’t either. Never be afraid to be proactive with your health…It’s not wrong to say to your doctor… ”This is my symptom…this is what I read about it…this test seems to provide clarity…is there a reason I should not get the test?” Until next month… Get well… Stay well.
Get Yourself to the Fair | September 5 2015
Dr. Barry
I had an article ready to go but I was then reminded that the New York State Fair opens up soon. As a dedicated health professional I would be remiss if I didn’t have some diatribe against the artery clogging junk to eat at the fair. In fact, I know I wrote about this exact same issue previously…I could just go back and cut and paste and who would know or care. Sorry, that’s not the way I roll. This is fresh off the cerebral cortex stuff but it will be very familiar. If I am going to preach about the same lifestyle issues over and over again I better have that patter down pat…so to speak.
 The important principles of how profound an effect that diet and exercise can have in your life and health don’t change but the ways to approach and illustrate them sure can. What can I say to those that don’t go to the fair? It boils down to this…anyone who doesn’t go to the fair is hiding something. That’s right, hiding something. Maybe they say, “It never changes,” but they are hiding the fact that they are too weak to make it around the fair on their own. Oh, maybe they are hiding the real fact from you but I think they are often hiding the reason from themselves as well…Not wanting to acknowledge their debilitated status. Maybe they say, “All the food there is unhealthy,” but again they are really hiding the fact that they have a hard time making food choices. If you call them on this they will say…no…I just don’t like the fair…to which I have always countered with, “What’s not to like?” but now I see I will have to ask, “What are you hiding?” All those people who say I went for 30 years in a row…What made you stop? Did you start doing something else instead?
The important principles of how profound an effect that diet and exercise can have in your life and health don’t change but the ways to approach and illustrate them sure can. What can I say to those that don’t go to the fair? It boils down to this…anyone who doesn’t go to the fair is hiding something. That’s right, hiding something. Maybe they say, “It never changes,” but they are hiding the fact that they are too weak to make it around the fair on their own. Oh, maybe they are hiding the real fact from you but I think they are often hiding the reason from themselves as well…Not wanting to acknowledge their debilitated status. Maybe they say, “All the food there is unhealthy,” but again they are really hiding the fact that they have a hard time making food choices. If you call them on this they will say…no…I just don’t like the fair…to which I have always countered with, “What’s not to like?” but now I see I will have to ask, “What are you hiding?” All those people who say I went for 30 years in a row…What made you stop? Did you start doing something else instead?
 The exaltation of the Fair is easy. First, is its proximity people! The damn fair is in our backyard and for that reason alone deserves a visit. As do the Zoo, the Everson, the MOST, Symphoria, Syracuse Stage, etc., but they are here year round. The State Fair is more ephemeral…here but a few days at the end of summer. Gone before you have even gone through your full list of reasons not to go. The Fair IS exercise! Walking, walking, walking…it’s exactly what I preach. You can walk miles at the State Fair and not see everything. There is indeed always something new at the Fair …maybe not something monumental but always something new. There is always a lot of educational stuff at the Fair and you know I preach about feeding your brain. Free music…and you know how I preach music therapy. The midway, the crazy deep fried “what-the-hell?”, the animal barns, the Native American area, all have their own allure.
The exaltation of the Fair is easy. First, is its proximity people! The damn fair is in our backyard and for that reason alone deserves a visit. As do the Zoo, the Everson, the MOST, Symphoria, Syracuse Stage, etc., but they are here year round. The State Fair is more ephemeral…here but a few days at the end of summer. Gone before you have even gone through your full list of reasons not to go. The Fair IS exercise! Walking, walking, walking…it’s exactly what I preach. You can walk miles at the State Fair and not see everything. There is indeed always something new at the Fair …maybe not something monumental but always something new. There is always a lot of educational stuff at the Fair and you know I preach about feeding your brain. Free music…and you know how I preach music therapy. The midway, the crazy deep fried “what-the-hell?”, the animal barns, the Native American area, all have their own allure.
The Fair IS diet! Rather it’s a chance to test and challenge your diet. If you plan ahead, you can easily modify your diet and exercise enough before and after the Fair that you can overindulge on your favorite fair food. Are you on some “diet” you have to adhere to rigidly to get results or do you have a “lifestyle” that allows you to go buck wild on the deep fry but then rein it in the next day. Why would you go to the fair and look for a salad?
 That’s not just silly its insulting! I couldn’t find a green salad so I had to settle for the Blooming Onion!? People Please! Now, there is one caution about the Fair. If you are over 50 you are crazy to go on any of those vomitorium rides. You have had your brain jostled and giggled around enough already…don’t add insult to injury. Go ahead and do the Ferris Wheel and try your luck at one of the squirt gun games but avoid all the upside down, back and forth stuff if you want to stay out of the nursing home. So, overall the New York State Fair is good for your health. I will pit the walking against the fair food any day…the secret of course is to make it any day…any one day…not every day! Get out of your rut. Try something new. Try something that you “used to do.” Keep up those traditions whatever they may be….well ok…drunk and disorderly is not a good tradition but you know what I mean. Get yourself to the fair and challenge yourself!
That’s not just silly its insulting! I couldn’t find a green salad so I had to settle for the Blooming Onion!? People Please! Now, there is one caution about the Fair. If you are over 50 you are crazy to go on any of those vomitorium rides. You have had your brain jostled and giggled around enough already…don’t add insult to injury. Go ahead and do the Ferris Wheel and try your luck at one of the squirt gun games but avoid all the upside down, back and forth stuff if you want to stay out of the nursing home. So, overall the New York State Fair is good for your health. I will pit the walking against the fair food any day…the secret of course is to make it any day…any one day…not every day! Get out of your rut. Try something new. Try something that you “used to do.” Keep up those traditions whatever they may be….well ok…drunk and disorderly is not a good tradition but you know what I mean. Get yourself to the fair and challenge yourself!
Don’t You Remember! | August 3, 2015
Dr. Barry
The experts claim that one in three Americans will suffer from Alzheimer’s disease. Suffering is a relative word because honestly most of the suffering done with Alzheimer’s is the suffering of the caregivers as the patient themselves is usually unaware of their condition. You suffer through cancer…you suffer through depression…your family members are the ones that suffer when you have severe memory loss. Alzheimer’s is listed as one of the top 6 causes of death in America but before it kills you it takes a toll on you, your dignity, your family, your bank account, etc. Dementia is probably the #1 diagnosis in the nursing home and therefore at $8,000 a month, per patient, it’s probably one of the most expensive diagnosis to treat on a national level. Maybe one of those wildly expensive chemotherapy agents are more expensive but usually they’re used for 6 weeks or 3 months whereas dementia can persist for decades.
I don’t actually use the term Alzheimer’s much…It’s really a diagnosis that can be made with brain evaluation at autopsy and it’s just a name…I prefer to call it by the more practical and less charged name…memory loss.
That’s what I see and that’s what I try to treat. You could call it Alzheimer’s, you could call it Binswanger’s disease, you could call it Lewy body dementia, you could call it senile dementia, you could call it multi-infarct dementia but the bottom line is the person has a functional problem with their memory, usually short-term more than long-term. They might remember the name of their second grade teacher but they sure don’t remember where they left the car keys or that they wrote two checks to the cable company and one to the gas company. There are some new and up-and-coming brain scans that might help decide whether you have in particular the typical Alzheimer’s changes, but it doesn’t matter much since the treatments are all the same. There is no good reliable blood work to aid in diagnosis. Diagnosing dementia is like diagnosing Parkinson’s. It’s best done by the same observer evaluating the patient over time and seeing what changes occur. Unfortunately, in the modern doctor’s office the typical patient can get in and get out and be quite demented but not picked up by the doctor if he doesn’t ask the right questions. In an office visit with the doctor checking the blood pressure, checking the meds, checking the cholesterol and attending to any issues with the insurance company it’s hard to step back and ask “by the way can you tell me the name of the last 3 presidents? By the way can you remember these 3 words and draw me o’clock etc?” It is not particularly hard to do. You just have to have the time and interest… I have seen many people that were really having a lot of trouble with their memory before it was picked up by their healthcare professional because they didn’t think to ask the right questions. You don’t require a psychologist, or a neurologist, or any specialist to diagnose dementia.
 So dementia is diagnosed by asking patients questions. You can use formal testing like the Mini-cog, or the MMSE, or the SAGE questionnaire, or you can diagnose it informally. Once you look for it, it’s not hard to diagnose. On the other hand many people have mild cognitive impairment and never go on to dementia and it is hard to determine who will progress and who will not, and that’s why it is best managed over time by the same professional doing serial observations.
So dementia is diagnosed by asking patients questions. You can use formal testing like the Mini-cog, or the MMSE, or the SAGE questionnaire, or you can diagnose it informally. Once you look for it, it’s not hard to diagnose. On the other hand many people have mild cognitive impairment and never go on to dementia and it is hard to determine who will progress and who will not, and that’s why it is best managed over time by the same professional doing serial observations.
Now, the treatment for dementia is unfortunately quite limited. None of the current prescription medications cause significant and sustained improvement in cognition. The best we can say is that these medicines keep the patient as they are, and delays deterioration, but even the most ardent user of these medicines, if they look at the literature, realize they lose their efficacy within a year or year and a half. I wanted to be known as a very aggressive dementia doctor and so when the NIH recommended that we use Aricept and then add Namenda that’s what I did. I happily told patient’s I was following the NIH recommendations proving to them that I was an up-to-date well-informed physician. The only problem was this combination didn’t really work well for the vast majority of patients I treated. There might have been a patient here and there that the family said they noticed some improvement temporarily, but it wasn’t common. Additional experience with these medicines over time has continued to disappoint. Not only did these drugs not make a big difference…they also had side effects. My experience has shown me that in point of fact the benefits are quite minimal and the side effects are real, not dangerous but real. I have had many patients stop these pills and either did not deteriorate further or improved off the medicines, so my view of prescription treatment for dementia has been leavened by experience over time. There are also 2 medical foods/nutritional supplements to treat dementia as well and they include Axona and Cerefolin NAC. I like the idea that there would be some vitamin you could use that might actually have a clinical effect because I think there are less side effects with these prescriptions then there are with the other drugs mentioned previously. Unfortunately, these nutritional supplements are not usually covered by insurance because they are considered vitamins but they are not available in GNC or Natur-Tyme as they require a prescription from the doctor. Once again although individual families will say this medicine helped or that medicine helped they have not been overwhelmingly successful. Worth a try: yes. Guaranteed to work: absolutely not. I have absolutely no confidence in any nonprescription supplements that are available in the nutrition stores and vitamin stores. Completely unproven and potentially dangerous! Show me a single study done in America using human beings that show some improvement in a double blinded study and I will happily change my tune. So unfortunately, our current armamentarium is quite limited when it comes to treating Alzheimer’s/memory loss and therefore we are left with trying to prevent it, which I think in the long run is much more important…
There are obvious risk factors for dementia and they include smoking, diabetes, hypertension, and being inactive. There are genetic risk factors as well but there is nothing you can do about your genes so we focus on the modifiable factors. So yes, you can directly diminish your risk of dementia by not smoking, not drinking excessive alcohol, controlling your blood pressure and controlling your sugar. I prefer to focus on the couch potato aspect because the studies show that this is one of the most important modifiable risk factors. Besides exercise helping your cholesterol, your blood pressure, your joints, your mood, your fall risk, etc. physical exercise cuts your risk of dementia. Mental exercises are also touted to prevent dementia but the evidence that supports that is very slim. Physically pumping more blood to the brain works…mentally challenging your brain hasn’t been shown to work. It just makes sense to me that if you can open up the arteries to your brain with exercise you can get a little better blood flow and therefore a little better function from the brain. Studies have not shown that mental exercises have a basic and lasting impact but studies have shown that physical exercise seems to be associated with a lower risk for dementia. The mature patients that I see on a regular basis would benefit from exercise for many reasons not just the dementia component. People may be afraid of a heart attack or stroke in some vague way but the fear of dementia seems to strike a stronger chord. They take it a little more personally because they know someone who’s had the problem. Still, knowing about it and actually doing something about it are two different things. Get up off the couch and take a walk regularly…walk over to the local Nursing Home and that will provide you much better motivation than I can with this article. If walking through the halls of the nursing home doesn’t motivate you to get moving while you still can nothing will!
So memory loss can be a terrible problem with life changing consequences for the entire family…meds so far have little effect…but you are not helpless against this scourge…In fact you don’t need special tools, expensive tests, or exotic supplements to ward off memory loss. You just have to move it or lose it. Move your body to prevent losing your mind. So what or who are you waiting for? Until next month…get well…stay well.
Drop Dead! | July 2, 2015
Dr. Barry
I often use this line…“I like you…I hope you drop dead!!” Immediately, most people are, of course, taken aback until they think about it for a bit. I didn’t say drop dead right here and now. I said drop dead…eventually. Think about it for a minute and you will find yourself…reluctantly as always, agreeing with me. What are your eventual options? You could just keel over shopping or at dinner OR end up dying after a long and difficult fight with cancer. You could just die quietly in your sleep OR spend your last days drooling over yourself demented in the nursing home. Now, with this perspective I think you’ll agree that a short painless expiration is preferable to a long lingering finish. In essence…dropping dead, when you consider the other options, is quite desirable.
 What brings this issue to mind this month are two separate articles in the medical literature recently as well as my wife having to take a CPR class for her new job. I have been feeling pretty good about my medical pronouncements recently because things that I have been saying for years are finally making front page news in the Journal of the American Medical Association and in the New England Journal of Medicine and in the Cleveland Clinic etc…From Charles Krauthammer writing in the Washington Post about the dissatisfaction of doctors, to articles in JAMA about how diabetic care has to be personalized to the patient, to articles in the NEJM about the difficult issue of pain management with chronic opioids, and including two articles regarding CPR.
What brings this issue to mind this month are two separate articles in the medical literature recently as well as my wife having to take a CPR class for her new job. I have been feeling pretty good about my medical pronouncements recently because things that I have been saying for years are finally making front page news in the Journal of the American Medical Association and in the New England Journal of Medicine and in the Cleveland Clinic etc…From Charles Krauthammer writing in the Washington Post about the dissatisfaction of doctors, to articles in JAMA about how diabetic care has to be personalized to the patient, to articles in the NEJM about the difficult issue of pain management with chronic opioids, and including two articles regarding CPR.
The first article was about improvements in CPR but when you drilled down to the actual numbers what you find is that even in the best of hands out of hospital resuscitation gives you less than 1 in 10 chance of surviving to the hospital. Note this is not intact survival. It’s having a heart beat when you reach the emergency room. “Survival” often means living with major brain damage. The 1 in 10 chance is of course very optimistic…the more realistic number is that less than one person in 20 will survive long enough to reach the emergency room doors. They never talk about the part wherein most people who have been successfully resuscitated are never the same again. This is not the way I want to go!
Let me take a moment here because I know a lot of people are going to respond angrily to this article. They’re going to say they saw someone or know someone who was successfully resuscitated. Well, it’s got to work right sometime but I think when someone collapses in the store people rush to pound on their chest… they could have just had a faint or a seizure…but in the stress and urgency of the moment they get CPR even if they don’t really need it…then they wake up and it’s a “save from CPR.” Don’t take my word for it…ask any ambulance attendant or an emergency room nurse about the effectiveness of CPR. How often do people with no heartbeat get successfully brought back to life with no significant deficits?
 Also, don’t get me wrong I am a big believer in defibrillation but not CPR. If someone collapses due to very irregular heartbeat called ventricular tachycardia or ventricular fibrillation…hooking them up to the defibrillator can restore a regular rhythm quickly and easily and the person will usually not have significant brain injury. This is a whole different kettle of fish from pounding on someone’s chest so hard which, if done properly, causes rib fractures and other injuries even as you try to save the person’s life.
Also, don’t get me wrong I am a big believer in defibrillation but not CPR. If someone collapses due to very irregular heartbeat called ventricular tachycardia or ventricular fibrillation…hooking them up to the defibrillator can restore a regular rhythm quickly and easily and the person will usually not have significant brain injury. This is a whole different kettle of fish from pounding on someone’s chest so hard which, if done properly, causes rib fractures and other injuries even as you try to save the person’s life.
The second article on CPR was an editorial commenting that even in the hospital with the plethora of trained personnel the survival to get to the ICU was only 20% and again these are people who survived just to be transferred to the ICU. They don’t give out the figures for the extent of brain damage. This article said we should be doing less CPR in part due to financial considerations because the last 90 days of people’s lives can be frighteningly expensive but my rejection of CPR is not based on finances. I am a doctor not an accountant. My point is that there is a time and a place for everyone to be born and for everyone to die. For us to attempt to intervene usually does not end well for the patient nor for the family for that matter.
I call for a respect of death. If you are religious, the line I would use is to say “If the Lord calls you home which He will do eventually, and He gives you an express pass by having you collapse suddenly and painlessly in your sleep let’s say…Why would you or anyone else want to delay it?” If you’re not religious, I point out the basic facts that when your heart gives out your brain and kidneys usually follow and instead of a dignified moment of silence for you as you pass you get instead days or weeks of slowly worsening in the intensive care unit until some doctor’s sad duty is to suggest to the family it’s time to turn the machines off and let the patient meet their end peacefully. It doesn’t have to be that way. We should have a better respect for the quality of healthy living and not try to deny aging or death. Of course this is a hard sell in a country obsessed with youth and looks. We have all kinds of celebrations when people give birth and I’m not saying we should celebrate death but we certainly should acknowledge it in a less desperate manner than we do today.
Again there are always exceptions and cold water drowning etc. may justify CPR but for the run-of-the-mill patient who collapses in the parking lot I personally don’t feel that I am doing them any favors when I perform CPR. I know it’s very unlikely to result in any quality time for the patient. For a doctor trained to help people, not taking action is difficult but I’ve learned through a fairly long career so far that sometimes the best action is no action.
 As you know CPR, until recently, has involved pounding on the chest and attempting to breathe for the person but the American Red Cross is abandoning the concept of breathing for the patients stating that pounding on the chest alone produces the same results as pounding and breathing. I propose to you that the reason they abandoned the breathing part of CPR is because it doesn’t work well, but then again I don’t believe that the pounding on the chest works well either. If a procedure works only one time out of 20 that to me is not successful.
As you know CPR, until recently, has involved pounding on the chest and attempting to breathe for the person but the American Red Cross is abandoning the concept of breathing for the patients stating that pounding on the chest alone produces the same results as pounding and breathing. I propose to you that the reason they abandoned the breathing part of CPR is because it doesn’t work well, but then again I don’t believe that the pounding on the chest works well either. If a procedure works only one time out of 20 that to me is not successful.
You know I love my mama but I hope she passes quickly and painlessly when her time finally comes. Making someone a Do Not Resuscitate or having a MOLST form or Health Care Proxy gives patients the chance to have some say in what’s done when they get sicker. Making someone a DNR doesn’t mean put them in a corner and ignore them. It means that when it’s obvious to health professionals and family alike that the end is near we treat the patient with dignity and not as a piece of meat. That people are given the option to die at home or in a comfortable setting surrounded by their family and friends, not being subjected to what I think is cruel and unusual punishment in a frantic environment during their final moments.
Many times my job as a geriatric specialist is to tell people that less may be more. Maybe you need less medicines. Maybe you need less testing at a certain age. Maybe we should look ahead and make plans for that final day whenever that might come. That’s something that each patient and doctor should decide together. You didn’t have any choice about how you came into this world but at least here in America you have plenty of choices about how you’re going to go out. A little planning done ahead of time can make a huge difference.
No Butts About It! | June 3, 2015
Dr. Barry
 I received a lot of responses to my Bitch Bitch Bitch column from last month. One person asked me if was ever going to write about real medical issues as the column is labeled Preventive Medicine. So here you go Stan!
I received a lot of responses to my Bitch Bitch Bitch column from last month. One person asked me if was ever going to write about real medical issues as the column is labeled Preventive Medicine. So here you go Stan!
There’s a new player in town…cancer town that is. That player is a test called Cologuard. Colon cancer is the second leading cause of cancer death in men and women so it’s obviously important. This is not some obscure disease we are talking about like the Pustular Psoriasis of Von Zumbusch or the Spreading Depression of Laeo. This is a disease that is killing someone in your family or your neighborhood. And colon cancer is not a quick easy death. There is much we can do to you and for you before the end. The NIH spends roughly 270 million dollars a year just funding studies of colon cancer. This figure does not include the detection of cancer, the treatment of cancer, etc. How do you put a number on the emotional toll of cancer? So, it’s a big deal when we have a new approach to detecting colon cancer.
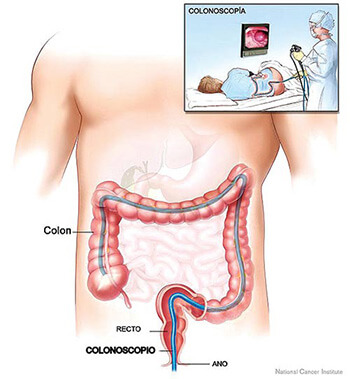
First, some facts and figures regarding colon cancer. The average American has a 5% risk of colon cancer in their lifetime. Another way of stating the same thing is that one person in 20 will get colon cancer. Men get cancer more than women but we don’t know why.The last year for which we have firm statistics is 2012 and approximately 25,0000 women and 25,000 men died of colon cancer that year. Cancer deaths are going down because of improved detection primarily from colonoscopy as far as we can tell. 90% of colon cancer incidents occur in people aged 50 and over. That’s why most people started having a screening colonoscopy at age 50. The important thing is to find the cancer while it can be excised simply without needing chemo or radiation, etc. Currently the #1 way to do this is with colonoscopy.
 A colonoscopy is the insertion of a flexible lighted periscope into your rectum and looking into your colon for any kind of cancerous or precancerous lesions. It’s not cheap. It’s uncomfortable enough that for most people it requires a sedating injection. The prep which is required for the test is often considered the worse part of the whole procedure. You need to get cleaned out so the doctor can see enough to be sure he didn’t miss anything. Many people dislike the prep more than they dislike the procedure. If the preparation isn’t good enough the colonoscopy might have to be repeated and / or they might resort to using an older technique like a barium enema. There is a new technique called the virtual colonoscopy which is basically a barium enema and a CAT scan but I never recommend this because #1 it is a lot of x-ray exposure, #2 the doctor could miss something and therefore you suffer because of a misdiagnosis, or #3 the radiologist could and often does say he thinks it could be a polyp and therefore you have to have a colonoscopy anyway. With virtual colonoscopy you still have to do a similar prep so virtual colonoscopy doesn’t work for me. There have been, up to now, a couple of other options including testing the stool for blood in the doctor’s office or in a take home preparation. I have given out well over 1000 of those packets and only got about 10 back, so that scenario has not played out well either. Testing for blood is not the same as testing for cancer.
A colonoscopy is the insertion of a flexible lighted periscope into your rectum and looking into your colon for any kind of cancerous or precancerous lesions. It’s not cheap. It’s uncomfortable enough that for most people it requires a sedating injection. The prep which is required for the test is often considered the worse part of the whole procedure. You need to get cleaned out so the doctor can see enough to be sure he didn’t miss anything. Many people dislike the prep more than they dislike the procedure. If the preparation isn’t good enough the colonoscopy might have to be repeated and / or they might resort to using an older technique like a barium enema. There is a new technique called the virtual colonoscopy which is basically a barium enema and a CAT scan but I never recommend this because #1 it is a lot of x-ray exposure, #2 the doctor could miss something and therefore you suffer because of a misdiagnosis, or #3 the radiologist could and often does say he thinks it could be a polyp and therefore you have to have a colonoscopy anyway. With virtual colonoscopy you still have to do a similar prep so virtual colonoscopy doesn’t work for me. There have been, up to now, a couple of other options including testing the stool for blood in the doctor’s office or in a take home preparation. I have given out well over 1000 of those packets and only got about 10 back, so that scenario has not played out well either. Testing for blood is not the same as testing for cancer.
Now for the new guy in town, and that’s Cologuard. Don’t get me wrong …colonoscopy is still the “gold standard.” That’s the test I get. But for people that are unwilling or unable to have a colonoscopy there is a new technique that’s called Cologuard. It involves simply sending a sample of your stool to the company where it is tested 11 different ways for any evidence of cancer. The test is 92% sensitive in the detection of cancers and that’s a very good number in medicine. The test is not perfect but neither is colonoscopy. The test report comes back simply negative or positive.. if it’s positive you need a colonoscopy…if it’s negative you are probably ok and can discuss what to do next, and when, with your physician. So if you have been neglecting getting your bowels checked for cancer it’s time to bring this article to your doctor and ask him what they think of this test and if it is for you. The test is for average risk people…it’s not meant for people who are known to be at increased risk for cancer, like people with a family cancer syndrome or patients with a history of colitis. Hopefully your doctor is familiar with the test and maybe a life will be saved. What a great way to start the summer. Until next time …get well and stay well.